











































Clinician Perspectives on Strategies to Improve Patient Maternal Immunization Acceptability in Obstetrics and Gynecology Practice Settings
Emory University School of Medicine (Frew, Randall, Fenimore, Omer); Emory University Rollins School of Public Health (Frew, Malik, Wilson, Omer); Johns Hopkins Bloomberg School of Public Health (Limaye, Salmon, Dudley); University of Colorado Denver (O'Leary); University of Colorado School of Medicine (Donnelly); University of Kansas Medical Center (Ault)
"[T]here is a need for more tools and training on effective communication approaches with pregnant patients about maternal and childhood vaccines, especially considering other persuasive influences surrounding women's decision-making during pregnancy..."
Early exposure to positive immunisation messages during pregnancy may make women (and their partners) more likely to vaccinate themselves and their infants. However, the barriers for increasing coverage of recommended maternal vaccines and addressing parental concerns for infant vaccines are complex and multifactorial. Guided by behavioural theories (Elaboration Likelihood Model (ELM), the Stages of Change Model, and the Systems Model of Clinical and Preventive Care), this study was designed to facilitate the introduction of a comprehensive maternal vaccine promotion strategy in obstetrics and gynaecology (ob-gyn) clinical settings. Its specific aim was to identify a set of clinic, provider, and staff-related attributes and facilitators that could be used for intervention development and implementation.
The researchers conducted in-depth interviews with 24 healthcare providers (i.e., physicians, nurse practitioners, midwives) and clinic/practice staff (i.e., nurses, medical assistants, practice managers) from selected urban and suburban ob-gyn practices in Georgia and Colorado, United States (US) in 2015. Qualitative analyses included Pearson correlation tests to evaluate patterns and relationships within the data to determine themes.
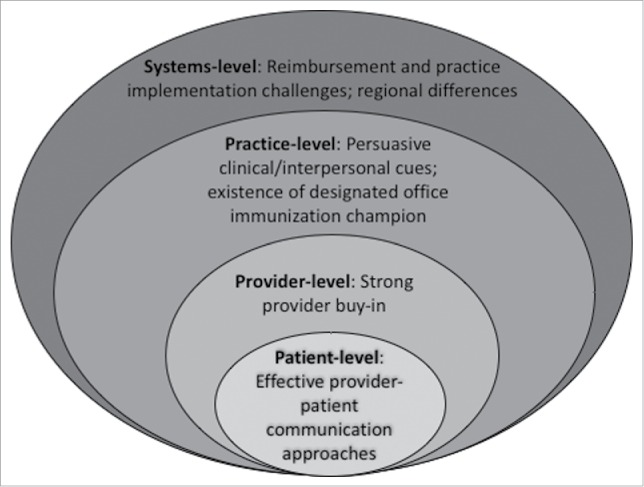
The researchers identified 6 major themes aligned with a socioecological model (see above) that emerged from the data collected from this sample; they are elaborated using quotations from participants in the study. In brief:
- Strong provider "buy in": The researchers found strong consensus among providers supporting maternal vaccination. They indicated that vaccine promotion and discussion with patients was a general established practice norm. Most of the providers claimed they were knowledgeable about the current recommendations and did their part to ensure that they passed the information along to their patients.
- The supporting role of clinical/interpersonal cues for vaccine promotion: The providers described the clinical environment as conducive for promotion of maternal immunisation. They discussed a need for specific types of education materials from credible sources and intentional placement of materials such as posters and brochures around the clinic to promote immunisation. The availability of designated sections on websites dedicated to this topic was inconsistent across practices; in other words, immunisation is not a prominent topic in many of their sites.
- Varying provider-patient communication approaches and its influence on maternal and paediatric uptake: Most of the providers said they approach the introduction and promotion of maternal immunisations through one-on-one discussions in clinical encounters. Specifically, they reported discussing immunisations with patients based on what they know the patient values so they can speak to their issues in a more salient manner.
- Regional attitudinal differences toward maternal immunisation - for example:
- The types of myths and issues providers encountered resulted from exposure to others in their local social networks who promulgate vaccine concerns and fears. These challenges are described as more difficult to surmount in Colorado compared to those in Georgia.
- Providers in Colorado were less inclined to challenge women's vaccine refusal after a maximum of three times, in contrast to those in Georgia, who did not indicate having such "hard stop" milestones on vaccine discussions.
- The Georgia practices described the challenges of working with limited English-speaking patients on the topic of maternal immunisation. Although they recognize there may be cultural beliefs deterring women from getting a vaccine, often these could be surmounted with clear, understandable dialogue between the provider and the patient.
- Reimbursement and practice implementation challenges: Managers in particular spoke about the conflicts they faced with providing patients with access to vaccines in the clinic, yet needing proper renumeration for the practice.
- Need for a designated office immunisation champion: Many expressed that the individual in this role was essential in promoting the messages presented concurrently though clinical cues (i.e., education materials in the waiting and treatment areas) as well as to reinforce the importance of immunisation through patient-provider conversations. However, very few of the providers described an actual designation of this role in their practice. For those practices that had such a champion, often this individual was identified as the attending physician.
In the researchers' estimation, these findings:
- Support other studies that speak to the importance of practice materials. As materials are widely available from several public health websites, practices could easily download communication materials to display in their waiting rooms and exam rooms. As waiting times were seen as an opportune moment to provide educational material, practices could provide vaccine-related information, such as brochures or vaccine information summary sheets, once a patient checks in with the reception team. This allows the patient to read through the material before interacting with the provider, thus priming the vaccine-related conversation.
- Suggest there is a need for providers to use communication materials that are tailored to the patient, as this forms a basis for a trusting relationship. For example, patients who have declined vaccines several times may require different persuasive techniques than those that are having an initial conversation with their provider about vaccines. Providers should communicate in a way so that patients feel as though their concerns have been addressed through open questioning and through an agreement between the patient and the provider about the nature of the concern. By establishing empathy, providers can allay patient concerns and fears, which, in turn, can build trust.
- Reflect needs for immunisation champion identification, training, and support, as this person plays a role in establishing the norms within a particular practice, leads efforts to improve immunisation delivery, and assists in ensuring that providers are able to resonate with parents on a personal level. Previous studies have shown that immunisation champions can improve vaccination rates. Future research could explore which staff makes the most effective immunisation champion and what sort of training is most appropriate.
Human Vaccines & Immunotherapeutics. 2018; 14(7): 1548-57. doi: 10.1080/21645515.2018.1425116
- Log in to post comments