











































Using Behavioural Science and Human Centered Design to Boost COVID-19 Vaccination
"Within this dynamic COVID context and rapidly evolving response, it is critical for the state and key stakeholders to keep up with the perceptions, sentiments and drivers of behaviours on the ground. The demand for COVID testing and vaccination is situated within this dynamic."
In the context of the COVID-19 pandemic in India, Final Mile and PATH undertook a research-based process using a behaviour science and human-centred design (HCD) approach to understand barriers to uptake of COVID-19 vaccines and to then design interventions to drive vaccine uptake in Punjab and Maharashtra. Among the project objectives:
- Understand the conscious and non-conscious drivers of hesitancy or refusal towards COVID-19 vaccine for the first and second second shot; and
- Identify strategic levers for designing communication and service delivery protocols for boosting COVID-19 vaccine confidence in the intended population to drive uptake.
The research that informed this project was conducted in consultation with, and the with permission of, State officials of Maharashtra and Punjab, during the time period of March-July 2021, in Nagpur (urban and rural), Bathinda (urban), and Faridkot (rural).
The project process used HCD to ensure consolidating of existing knowledge, in-depth user research (with users and stakeholders), partnership with the State, and close collaboration with the PATH team to leverage their on-ground State and medical expertise to move from strategic insights to framing design intervention for uptake. It included:
- Stakeholder consultation and evidence review: (i) Interviews with PATH and State stakeholders to understand the service delivery design and existing communication strategy, to frame the key problem to be addressed, and to align design requirements; and (ii) a review of existing secondary literature and internal project reports.
- User research: 34 remote in-depth interviews with end users and 7 interviews with State nodal officers and stakeholders (frontline workers (FLWs), doctors, contact tracers, vaccination staff) across Nagpur, Bathinda, and Faridkot.
- Overall, this process revealed that the formal government communication around the vaccine has been perceived to be clinical, operational, generalised, and not tailored to individuals' different needs. Therefore, individuals default to existing vaccine mental models and seek out information from informal news channels (e.g., social media) and others' "lived experiences", which has led to incorrect beliefs around the purpose of the vaccine (protection vs. prevention vs. treatment), misinformation, and perceived high negative consequences of taking the vaccine. The vaccine decision is based on a feeling of risk and reward than an objective analysis. The risks of taking the vaccine are high (due to the salient negative stories) with low to no reward, and the rewards of inaction are high, with low risk; therefore, inaction is favoured. This is not an individual decision; rather, it is influenced by family members, friends, and employers. In short, the research found that the decision of not taking the vaccine is arrived at based on how the COVID-19 context is perceived, the norms around COVID-19 vaccination, and the feelings of risk and reward. These decisions manifest as 4 types of negative narratives around why people do not want to take the vaccine:
- Vaccine is irrelevant: "I am healthy, and I don't need the vaccine."
- Vaccine is scary for me: "I already have health issues; what if they get worse after the vaccine?"
- Vaccine is a "costly" alternative: "I am fine now, I am keeping myself safe now, I can't take a chance with the vaccine."
- Vaccine is a scam: "I think the COVID-19 vaccine is a scam, so there is no reason for me to take it.
- Overall, this process revealed that the formal government communication around the vaccine has been perceived to be clinical, operational, generalised, and not tailored to individuals' different needs. Therefore, individuals default to existing vaccine mental models and seek out information from informal news channels (e.g., social media) and others' "lived experiences", which has led to incorrect beliefs around the purpose of the vaccine (protection vs. prevention vs. treatment), misinformation, and perceived high negative consequences of taking the vaccine. The vaccine decision is based on a feeling of risk and reward than an objective analysis. The risks of taking the vaccine are high (due to the salient negative stories) with low to no reward, and the rewards of inaction are high, with low risk; therefore, inaction is favoured. This is not an individual decision; rather, it is influenced by family members, friends, and employers. In short, the research found that the decision of not taking the vaccine is arrived at based on how the COVID-19 context is perceived, the norms around COVID-19 vaccination, and the feelings of risk and reward. These decisions manifest as 4 types of negative narratives around why people do not want to take the vaccine:
- Development of strategic insights: Final rigorous analysis and synthesis of the user research to build a strategy to highlight the barriers to COVID-19 testing, in order to understand levers for behaviour change.
- Co-design: Workshops with PATH stakeholders to prioritise and develop design concepts on the strategic levers identified to drive uptake of COVID-19 testing and COVID-19 vaccine.
- Intervention concept development: creation of intervention concepts, based on the strategic insights and workshop inputs. The 4 strategic directions to drive vaccine uptake include:
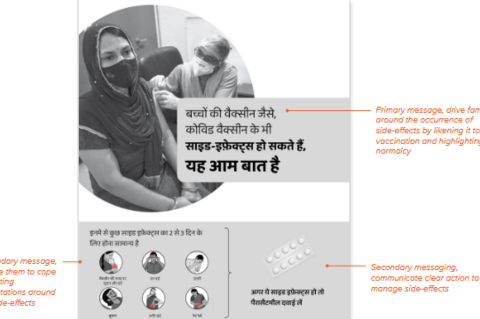
- Addressing information gaps: A barrier-focused communication campaign focused on the relevant emotional benefits of taking the vaccine, customised to the 4 barriers' narratives, above, and reframing side effects. Possible areas of emphasis: reframing uncertainty as an opportunity to act and creating positive stories to reduce the dissonance for those expecting prevention from the vaccine and yet may get infected between the first and second doses of the shot (furthermore, negative family and social norms associated with COVID-19 and the vaccine act as barriers, even if the first dose has been taken). Potential channels: posters in frequented locations such as grocery shops, hoardings, wall paintings, newspaper ads, radio, social media, and phone caller tunes. Sample strategy: using realistic illustrations of relatable people who are representative of urban/rural and the State.
- Managing myths and misinformation: Undertaking localised community misinformation management of adverse events following immunisation (AEFIs) and related narratives by creating a local committee leveraging trusted people in the community to track and then reduce spread of misinformation. Recommended process for debunking vaccine myths: (i) State the fact: Lead with a few words by stating a relevant fact about the vaccine that helps in understanding what the vaccine is. (ii) State and debunk the myth: Repeat the myth only once, and state it as false. Explain why the misinformation is usually considered to be correct in the first place, and why it is now clear that it is not the correct information. (iii) Reinforce facts: Restate the fact again, so the fact is the last thing people process.
- Enabling better trade-offs - A customised communication approach for field-level workers that involves transforming the one-on-one FLW vaccine conversation into a new approach that starts with an understanding of specific barriers and myths and provides customised benefits to drive uptake (e.g., providing incentives to build coping and creating costs for inaction). This approach can be conveyed through short, engaging WhatsApp videos that feature an experienced ASHA worker talking through the new approach to aid conversation and an example conversation. These videos will be supplemented with "reference sheets" shared on WhatsApp (or printed for easy reference).
- Encouraging advocacy and adherence - Building on existing vaccination site guidelines from a behavioural perspective to ensure a uniform positive experience and counter barriers at the 3 stages of the vaccination process: registration, vaccination, and waiting room. The messaging involves ensuring adherence by roadmapping next steps, driving second-shot commitment throughout the journey, and extending advocacy to the family. For example, the Family Protection Card aims to extend vaccine uptake from only the self to the family. This intervention aims to convey the emotionally salient vaccine benefit to drive decision confidence, drive commitment to the date for the second dose, and encourage vaccination among close and extended family members.
The study identified 12 interventions in total and detailed one key intervention addressing each of the strategic directions. (For more details on these interventions, see Using Behavioural Science & Human Centered Design to Boost COVID-19 Vaccination: Insights and Strategic Interventions [PDF].)
- Rapid testing of design concepts: Rapid testing of design concepts among 25 users who had expressed barriers to COVID-19 vaccination and stakeholders (Panchayat members, informal doctors, State nodal officers, accredited social health activis (ASHA) workers, vaccination staff) for feedback on the acceptance, feasibility, and comprehension of intervention concepts.
- Final intervention concepts and report: Creation of a detailed design brief and concepts for the State government to implement the interventions for driving COVID-19 Vaccine confidence and uptake.
Immunisation and Vaccines, COVID-19
According to Final Mile, as PATH works closely with the State of India, their priority is on driving vaccination uptake. While a certain level of vaccine hesitancy in the population is to be expected, the indications of the scale of it for COVID-19 vaccination are alarming. Information overload around the pandemic is part of the reason why people's perceptions of efficacy and risk are deviating from established trends and patterns. Some attributes of the vaccines themselves, such as minimal adverse effects, high efficacy, and a longer immunity period, may reduce the hesitancy. Nonetheless, much of the hesitancy will have to be addressed at the level of specific beliefs, attitudes, and trade-offs of different segments of the population. While survey data and other studies are important to understanding overall hesitancy, there is a need for a behavioural science and HCD-led approach to identify strategic levers that can be used to design the communication campaign and service delivery design for vaccine rollout.
Final Mile, PATH
Using Behavioural Science & Human Centered Design to Boost COVID-19 Vaccination: Insights and Strategic Interventions [PDF], July 13 2021; and Project Brief: Using Behavioural Science & Human Centered Design to Boost COVID-19 Vaccination: Insights and Strategic Interventions [PDF] - both accessed on August 30 2021. Image credit: Final Mile and PATH
- Log in to post comments