











































Leapfrogging with Technology: Introduction of a Monitoring Platform to Support a Large-scale Ebola Vaccination Program in Rwanda
Johnson & Johnson Global Public Health (Mc Kenna, Masyn, Willems, De Paepe, Rutten); Rwanda Biomedical Centre (Mazarati, Sayinzoga); Project San Francisco/Center for Family Health Research, Kigali, Rwanda (Karita, Nduwamungu, Mazzei, Nyombayire, Ingabire); Grameen Foundation (Amponsah, Egoeh); Johnson and Johnson Health and Wellness Solutions, Inc. (Ezeanochie)
"...irrespective of the disease, successful vaccination campaigns rely on communication, community engagement and technology..."
Biometric and mobile messaging technologies have been increasingly used in public health interventions to identify individuals and communicate with the public, respectively. In light of continued outbreaks of Ebola virus disease (EVD), and given the population flow between Democratic Republic of the Congo (DRC) and Rwanda, the Rwanda Ministry of Health initiated a preventive vaccination campaign called Umurinzi, which means "guardian" in Kinyarwanda, the local language. Supported by a vaccination monitoring platform (VMP), the campaign aimed to vaccinate approximately 200,000 people from Rwanda's Rubavu and Rusizi districts with a 2-dose regimen. Approximately halfway through the vaccination programme (having administered more than 100,000 people with at least one dose), this article describes VMP implementation, along with its challenges and learnings.
The vaccination campaign commenced in Rwanda in December 2019. Vaccination sites were set up in 13 existing healthcare centres as well as pop-up vaccination clinics in tents at the border in order to increase accessibility to the campaign. All participants were provided with a fact sheet detailing the vaccination campaign.
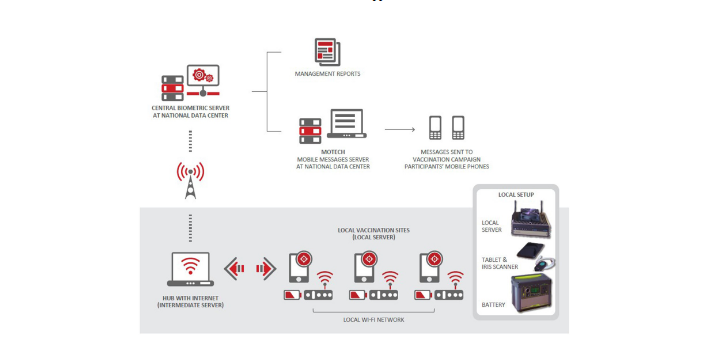
VMP equipment was transported to each healthcare centre in rugged cases, specifically designed to protect against harsh usage conditions. The platform was designed to operate with minimal infrastructure and at sites lacking electricity and internet connectivity; the back-up battery packs provided up to 8 hours of power.
The VMP encompasses: biometric identification (iris scanning), a telephone messaging-based engagement tool, and an interactive reporting dashboard. The VMP collects participant registration data, which are used to track participant adherence to both vaccine doses. The platform provided data regarding the operational, behaviour science, and management teams of the Umurinzi campaign in order to maximise vaccine coverage and compliance as the campaign progressed.
Continued engagement with campaign participants via mobile phone voice messaging and texts following their initial health centre visit was designed to ensure they returned for the second dose. Mobile phone technology (MOTECH, an automated phone messaging and data collection system) was used to communicate key information. Voice messages recorded in Kinyarwanda were sent to participants via voice call, followed by an automated SMS text, also in Kinyarwanda. The message and voice call content was developed based on empirical evidence from the literature that identified the determinants of vaccine acceptance, adherence, and hesitancy in sub-Saharan Africa. Reports on call completions and listening patterns were also generated to help the clinical team understand if additional community engagement was needed. On average, participants who answered the phone listened to 95% of voice recorded messages. In addition, in 93% of cases, participants listened to 90% or more of the message.
The principal metric collected by the VMP reporting dashboard was the overall uptake of the first and second doses of the vaccines. Data were collected in near real time during the campaign, such as the number of vaccines administered by age group, gender, and location. Details about vaccinations given to date are provided in the article based on these data.
The article describes some of the challenges encountered and overcome during VMP implementation, including challenges with identification (i.e., iris recognition), challenges around collecting high-quality data (e.g., errors in the mobile telephone numbers recorded), challenges with data reporting (prevented through close collaboration between on-site personnel and the platform design team), challenges with software updates (which required a reliable internet connection), and challenges when participants did not have a mobile phone (overcome through use of participant campaign cards highlighting the date of the next vaccination visit, for example).
The researchers suggest that, in many countries where national identification (ID) cards are not available/misplaced/illegible, biometric identification of patients can be a practical option to support healthcare campaigns worldwide. This method of identification was well received, with no participants declining this ID step. Furthermore, biometric identification advantages were found to be easy to use when accompanied by a strong "train-the trainer" framework and were able to fully function with limited internet connectivity.
In conclusion: "The Umurinzi campaign was successfully supported by the use of the VMP: biometric identification, a reporting dashboard, and mobile messaging functionality, demonstrating the feasibility of a preventive two-dose Ebola vaccination program. The campaign also provided insights into the ways in which community education strategies and mobile communication can maintain engagement and support participant compliance. Similar VMP approaches are feasible to help future vaccine campaigns leapfrog into a new era that is data driven and more insightful in terms of impact."
Human Vaccines & Immunotherapeutics 2021, Vol. 17, No. 9, 3192-3202. https://doi.org/10.1080/21645515.2021.1920872.
- Log in to post comments